
Here is the idea worth carrying through this whole piece: tesofensine does not have a “good effect” and a separate “side effect.” It has one effect, on one small set of brain chemicals, and what looks like a benefit from one angle looks like a risk from another. Once that clicks, the rest of the science stops feeling like a list of disconnected facts and starts feeling like one story told twice.
This is a plain explainer, not a sales pitch. Nothing here is for sale. Every claim traces back to a study you can open and read for yourself.
A quick refresher on how neurons talk
Neurons pass messages across tiny gaps called synapses. One neuron releases a chemical messenger, a neurotransmitter, and that molecule drifts across the gap to dock onto the next neuron. Once the message lands, the brain needs to clean up, sweeping the leftover neurotransmitter back out of the gap so the synapse is ready to fire again. It does this with transporter proteins that act a bit like tiny vacuums, pulling the chemical back into the neuron that released it. That cleanup step is called reuptake.
A reuptake inhibitor jams the vacuum. With the pump blocked, the neurotransmitter lingers in the gap longer and keeps nudging the next neuron. The signal gets stretched out. This is the same basic trick an SSRI antidepressant uses on serotonin alone. Keep that comparison nearby, because it explains a lot of what follows.
Not one vacuum, three
Tesofensine, a small molecule from a family called phenyltropanes (it carried the lab code NS2330 during development), does not jam a single pump. It jams three at once: serotonin, norepinephrine, and dopamine. That is why researchers call it a triple monoamine reuptake inhibitor. All three chemicals linger longer, together, all the time the drug is active.
That triple action is the whole story of the compound. Serotonin leans toward mood and fullness. Norepinephrine drives alertness and a good share of the body’s cardiovascular reflexes. Dopamine handles reward, motivation, and movement. Turn all three up together and the effects fan out widely: some are the intended win (less hunger), and some are the price tag (a quicker pulse).
Tracing the appetite effect back to its source
So why does turning up these chemicals mean eating less? The preclinical work has actually mapped this fairly precisely.
A 2010 study in Neuropsychopharmacology gave tesofensine to obese rats and picked apart which signaling pathways carried the appetite-suppressing effect. It landed mainly on alpha-1 adrenergic signaling (part of the norepinephrine system) and dopamine D1 receptors. The proof was direct: block the alpha-1 receptor and the appetite effect nearly disappeared; block D1 and it was partly reversed [P4].
Human brain imaging backs this up. A 2014 PET study in European Neuropsychopharmacology measured how much tesofensine occupied dopamine transporters in living human brains and found the occupancy rising with dose, reaching roughly 77% in the striatum at the highest dose tested [P3]. That is a meaningful amount of dopamine-system involvement for a weight drug, and it confirms in people what the rat studies suggested: the appetite effect isn’t a mystery. It runs through specific, identifiable norepinephrine and dopamine pathways.
The same dial that quiets hunger also speeds the heart
This is the part that deserves a slow read, because it isn’t a separate side effect bolted onto the mechanism. It’s the same mechanism, viewed from the cardiovascular side. Norepinephrine is the body’s alertness chemical, tightly linked to heart rate and blood pressure. Stretch out norepinephrine signaling and you are, by definition, leaning on the exact system that speeds the pulse.
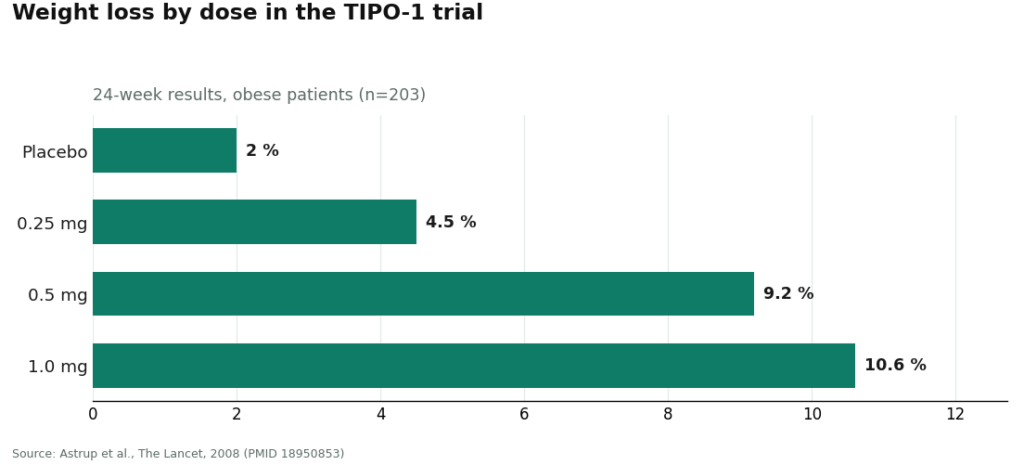
The numbers back this up. In the 2008 TIPO-1 Phase 2 trial, heart rate rose about 7.4 beats per minute at the 0.5 mg dose [P1]. A separate 2008 meta-analysis of earlier trials in Parkinson’s and Alzheimer’s patients found a similar dose-dependent rise, up to about 6.8 bpm, in people who weren’t even dieting, which tells us the drug itself is driving the change, not the weight loss [P2]. The highest dose tested, 1.0 mg, raised blood pressure enough that it was dropped from later development. Saniona, the drug’s developer, took this seriously enough to run a dedicated trial pairing tesofensine with the beta blocker metoprolol to try to blunt the heart-rate rise. That study flatly called heart rate “the most affected safety endpoint” of the drug, and it was halted over safety concerns before formally ending in 2019 [P5].
There isn’t anything mysterious in this. A compound that lengthens norepinephrine’s stay in the synapse is a compound that nudges the heart. The upside and the downside share a root cause.
Why it clashes with antidepressants
Two more things fall directly out of the mechanism, and the first is drug interactions. Because tesofensine blocks serotonin reuptake, it’s doing what an SSRI does. Combine it with another drug that raises serotonin and the effect compounds, which is the setup for serotonin syndrome, a dangerous overload of serotonin signaling. That is why tesofensine is flagged against SSRIs, SNRIs, bupropion, and stimulants, and why pairing it with an MAOI raises the risk of both serotonin syndrome and a hypertensive crisis [P5]. None of this is an arbitrary caution. It follows directly from two drugs leaning on the same system at once.
What we still don’t know about mood
The second loose thread is mood itself. Serotonin, norepinephrine, and dopamine are exactly the systems psychiatric medications target, so it’s fair to wonder how a drug touching all three affects mood. The honest answer is that the evidence here is thin, and thin for a specific reason: the obesity trials excluded people with known psychiatric disorders [P1]. That’s normal trial design, but it means the published safety data can’t really speak to how tesofensine behaves in people with a psychiatric history, who are precisely the people most likely to notice a mood shift. Mood effects remain a genuinely open question, not a settled one, and the mechanism itself is exactly why the question is worth asking.
Where the science actually stands
Zoom out and the mechanism explains the whole arc of this compound’s history. It began as a Parkinson’s and Alzheimer’s candidate, where hitting three monoamine systems at once was a reasonable idea, and the weight loss turned up as a side effect in those trials, more so in heavier patients, which is how the obesity program got started in the first place [P2]. The mid-stage efficacy result in TIPO-1 is real and solid. The cardiovascular cost is real and shares a cause with that efficacy. The drug interaction profile follows directly from the serotonin piece. And the mood data are thin for a clear methodological reason, not because the question was answered and came back clean.
What none of this settles is regulatory status. Tesofensine is not FDA-approved. In the US it sits classified as an investigational drug, and the confirmatory Phase 3 trial the original TIPO-1 authors said was needed hasn’t led to a US approval in the years since [P1]. Its furthest step anywhere is a favorable opinion from a Mexican regulatory technical committee (COFEPRIS) in early 2023, which is a procedural step in one country, not an approval.
Why the mechanism itself argues for supervision
Understanding the neuroscience leads somewhere practical, because the same biology that explains the effects also tells you exactly what needs watching. A drug that stretches out norepinephrine signaling needs someone checking heart rate and blood pressure. A drug that blocks serotonin reuptake needs someone checking the rest of a person’s medication list. A drug that touches three mood-relevant chemicals in people whose mood data are thin needs someone asking about psychiatric history. These aren’t generic warnings pasted onto any medication. They are the specific things this specific mechanism predicts will matter.
That is the case for getting tesofensine, where it’s used at all, through a licensed telehealth model rather than a chemical seller. FormBlends is a clear example of what that looks like in practice: a clinician evaluation first, a prescription written only when it’s appropriate, and dispensing through a licensed compounding pharmacy, typically running somewhere in the range of $90 to $300 a month depending on dose. One useful technical note that fits the chemistry: tesofensine is a small molecule, not a peptide, so it wasn’t caught up in the FDA’s recent restrictions on peptide compounding, and it remains available through licensed 503A compounding pharmacies with a prescription. The checks that model provides, a cardiovascular baseline, a review of other medications for the serotonin-reuptake interaction, careful dosing, ongoing monitoring, line up almost point for point with what the mechanism says matters. Patients who want to bring real data to a follow-up visit, logging dose and symptoms in between appointments (with something like the FormBlends tracker app, for instance), tend to get sharper conversations with their clinician out of it. That app logs information; it doesn’t prescribe anything and isn’t a checkout.
HealthRX (healthrx.com) belongs in the same supervised category, for the same reason: licensed clinical oversight up front, medication dispensed through proper pharmacy channels rather than sold as a raw research chemical. Choosing between the two mostly comes down to which is licensed in your state and which process fits your circumstances.
The alternative is the research-chemical route, where tesofensine shows up as a “research use only” powder with no clinician, no prescription, and no one checking in afterward. Everything the mechanism says needs monitoring goes unmonitored there. Nobody is tracking the norepinephrine-driven rise in heart rate. Nobody is checking your other prescriptions against the serotonin interaction. Nobody is asking about your mood history. And because the product isn’t reviewed by the FDA for identity, strength, or purity, you can’t even be fully sure what dose you’re taking. That isn’t a cheaper version of the supervised path. It’s simply the absence of the oversight the biology itself calls for.
Common questions, answered plainly
What does “triple monoamine reuptake inhibitor” actually mean? It means tesofensine blocks the transporters that clear three brain chemicals, serotonin, norepinephrine, and dopamine, out of the synapse, so all three stay active longer at the same time. An SSRI does this for serotonin alone; tesofensine does it for all three at once, which is why its effects spread so wide [P3][P4].
Why does tesofensine raise heart rate? Because norepinephrine plays a big role in cardiovascular tone, and tesofensine keeps norepinephrine active longer in the synapse. The same mechanism that curbs appetite also speeds the pulse, which is why heart rate rose about 7.4 bpm at the 0.5 mg dose in trials and was named the most-affected safety measure of the drug [P1][P5]. The benefit and the cardiovascular cost share one cause.
Why does it interact with antidepressants? Because it blocks serotonin reuptake much the way an SSRI does. Add another serotonin-raising drug and the effect stacks, raising the risk of serotonin syndrome, which is why it’s flagged against SSRIs, SNRIs, bupropion, stimulants, and especially MAOIs [P5]. That interaction is a direct, predictable consequence of the mechanism, not a mystery.
Is the mechanism actually well understood? Reasonably so. Animal studies traced the appetite effect mainly to alpha-1 adrenergic and dopamine D1 pathways, and human PET imaging confirmed dose-dependent dopamine transporter occupancy up to about 77% [P3][P4]. What’s genuinely unsettled is the regulatory picture: tesofensine remains investigational in the US, with no completed confirmatory Phase 3 approval [P1].
What is tesofensine and how does it differ from other weight-loss drugs?
Tesofensine is a small-molecule triple monoamine reuptake inhibitor, meaning it slows down how quickly the brain recycles dopamine, norepinephrine, and serotonin, all at once. That triple action sets it apart from older single-target drugs like sibutramine. It began life as a candidate for Parkinson’s and Alzheimer’s disease, and researchers only noticed the significant weight loss as a side effect along the way, which redirected its development toward obesity.
Is tesofensine a peptide, or is it chemically something different?
It’s not a peptide. Tesofensine is a small synthetic molecule, a phenyltropane derivative, putting it in the same broad chemical family as certain stimulant compounds rather than alongside the GLP-1 receptor agonist peptides like semaglutide. That distinction matters practically, since tesofensine works entirely inside the brain’s monoamine system rather than through gut-hormone signaling.
Does tesofensine actually burn fat, or does the weight loss come from eating less?
Most of the weight loss seen in trials seems to come from eating less, not from a direct boost to fat burning at the cellular level. Tesofensine does modestly raise resting energy expenditure through its effect on norepinephrine, but researchers consider appetite suppression the main driver. Calling it a “fat burner” gives the metabolic side more credit than the evidence supports.
Where can someone access tesofensine legally, and what should they watch out for?
Tesofensine isn’t FDA-approved, so it won’t turn up at a standard retail pharmacy. Some people access it through physician-supervised compounding pharmacies, such as FormBlends, where a licensed prescriber manages dosing and watches for cardiovascular effects like elevated heart rate and blood pressure. Buying it from research-chemical or supplement sites carries real risk: uncertain purity, zero medical oversight, and possible legal exposure depending on where you live.
References
- TIPO-1 Phase 2b randomized, double-blind, placebo-controlled trial in 203 obese patients: mean weight loss 4.5% / 9.2% / 10.6% at 0.25 / 0.5 / 1.0 mg vs 2.0% placebo over 24 weeks; heart rate +7.4 bpm at 0.5 mg; authors concluded the 0.5 mg result needs Phase 3 confirmation. Astrup et al., The Lancet, 2008. PMID 18950853. https://pubmed.ncbi.nlm.nih.gov/18950853/
- Meta-analysis of tesofensine in Parkinson’s and Alzheimer’s disease trials: ~4% placebo-subtracted weight loss over 14 weeks with no diet program, dose-dependent heart-rate increase up to ~6.8 bpm independent of weight loss. Astrup et al., Obesity (Silver Spring), 2008. PMID 18356831. https://pubmed.ncbi.nlm.nih.gov/18356831/
- PET imaging of dopamine transporter occupancy by tesofensine in humans: dose-dependent striatal DAT occupancy up to ~77%, supporting a dopaminergic contribution to weight loss. Appel et al., European Neuropsychopharmacology, 2014. PMID 24239329.
- Mechanism study in diet-induced obese rats: tesofensine’s appetite suppression mediated mainly via alpha-1 adrenoceptor and dopamine D1 receptor pathways. Axel, Mikkelsen, Hansen, Neuropsychopharmacology, 2010. PMID 20200509.
- Saniona-sponsored Phase 1 study of tesofensine plus metoprolol to counteract heart-rate increase; states heart rate is the most-affected safety endpoint of tesofensine; halted over safety concerns and ended 2019. NCT03488719.
- Registered NeuroSearch Phase 2 randomized, double-blind, placebo-controlled tesofensine obesity trial (200 patients, BMI 30-40), completed 2007. NCT00394667.



